Reference for patients and the medical community
Thinking about taking or prescribing disulfiram for Lyme & coinfections?
Read here and prepare FIRST for the safest and best outcome using this very effective medication!
What it treats:
Disulfiram has shown to be effective treating and or eradicating borrelia and babesiosis, aspergillus mold, vermicide, and possibly virus's per the HIV study. What studies we have are below to support this. Some patients report their bartonella symptoms can flare while on DSF, but how effectively it's killing it is yet to be known. None of this website or page is medical advice and for informational purposes only. This reference guide was made from what expert doctors with the most experience studying, publishing and using the drug have shared in treating persistent Lyme and coinfections with disulfiram (DSF). Talk to your treating physician about the use of any medication and check for drug interactions prior to starting including any THC or CBC products. All links are shared below for an all-encompassing reference guide to date.
“The tortoise will always beat the hare”, Dr. Daniel Kinderlehrer.
If you are sensitive to treatments, you can start prior to disulfiram by prepping the body for treatment. Incorporating a binder and detox protocol 2-3 x's a day is important to help the body flush the lymph and organs before we increase the load of die-off. Stay hydrated! Drink 2 oz of water every 15 minutes is a nice reminder to stay hydrated and free of constipation. Our brains love hydration too and you will have more energy and generally feel better. Binders are products that pull toxins from the body like activated charcoal, bentonite clay, cholestyramine, Enterosgel and G.I. Detox are some patient favorites. Take this away from food and supplements or medication at least an hour.
A good detox protocol might include infrared saunas (low EMF) a few days a week opposite to days you might do colonics/enemas. There are many ways to detox but some typical ways Lyme patients have benefited have been by the use of dual ionic foot baths, saunas, liver support, and juicing. Liver support might include milk thistle, ALA, glutathione, NAC, and coffee enemas. We want to support the liver to improve its function and efficiency. Liver damage is a rare side effect on DSF, but Lyme patients need to increase supporting the organs doing the most work ie, liver, gallbladder, and kidneys. Consider adding light rebounding if you’re able, to help lymph get moving; arms above the head for the best approach.
Any mold and candida treatment or heavy metal toxicity should be considered before DSF treatment. Test to check if these are at higher than normal levels and work the protocols to get them to a healthy level. It's also a good idea to ask your Dr. to check you for how high your histamine and cortisol levels are and treat you appropriately prior to adding DSF therapy that may increase die off, thus increasing inflammation and cytokine production. Antioxidants can be of help during DSF treatment but needs studied further. Supplements can contain metals that may bind with DSF and should be avoided.
Those can include:
Silver
Copper
Iron
Here's a link to Kristina's dedicated channel on Lyme for information about detox baths and other modalities to help you heal https://www.youtube.com/channel/UCWIlIK3C-J52644PKblX8hw. Detox baths are an inexpensive way to alkalize the body and lessen pain. Patients report this has been very effective for anything from fibromyalgia to brain swelling and migraines. Refrain from apple cider vinegar in your bath as it can react while on DSF. This varies per person. Any sauna work will INCREASE die off as it forces a fever. Some days maybe binders or Burbur/Pinella (Nutramedix.com) may be a better approach if you’re already experiencing a herx. We want to lessen that burden while treating tick-borne illness, not increase it. Another helpful tool would be to consider colonics or coffee enemas.
As to Dr. Kinderlehrer’s reference above, going slow on this protocol like a tortoise will always beat the hare who goes fast and hard. Patients tend to experience fewer toxic feelings of side effects and herxing working this approach he suggests.
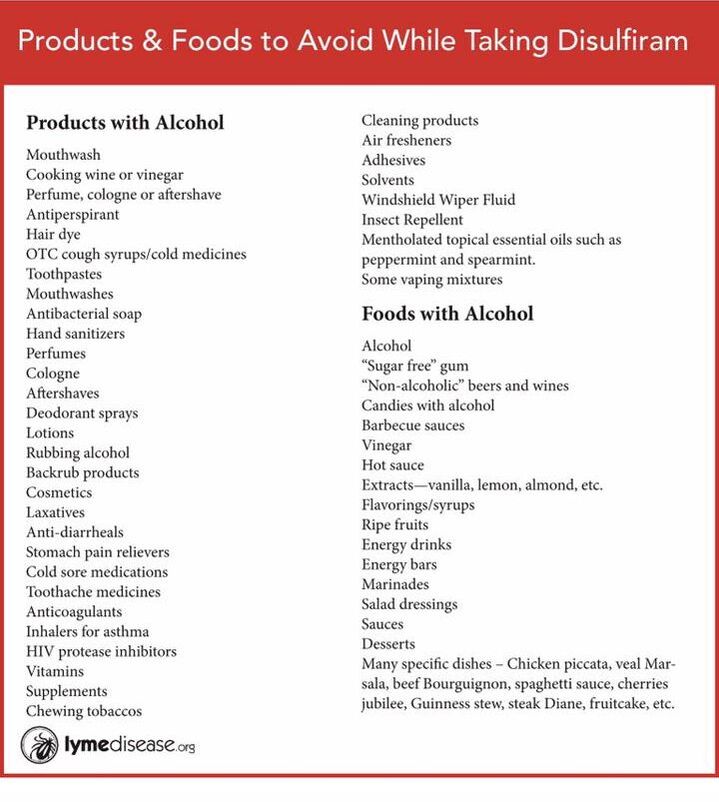
A few things to consider. Oxidative therapies like hBot and ozone can increase die off and cause herxing. We want to focus on one intervention at a time and refrain from increasing inflammation, treating with DSF just under a herx to avoid producing more histamine that can build upon the next dose. A good diet on DSF will vary depending on your sensitivities but thinking in terms of eating “whole foods” might help. Foods to avoid while on disulfiram is any alcoholic beverage, anything fermented like kombucha, rice, yeast and possibly even, probiotics. Ketchup, dressing, mustard and some soy sauce has vinegar, shampoo and lotions have alcohol. Some people are sensitive and react to rubbing alcohol when giving blood while others don’t at all. It’s best to not chance it but is an individual.
ACETALDEHYDE: Some vaping mixtures contain alcohol and should be avoided. Herbal tinctures, some stevia, vanilla extract, and homeopathy also sometimes contain alcohol. Check everything first in your kitchen and bathroom and eliminate your risk prior to starting your treatment. It will be easier to be successful when well-planned beforehand. Avoid any mentholated topical essential oils such as menthol, peppermint, and spearmint. Anything that ends in "ol" can contain alcohol like thiols. Overly ripe fruit can cause a DSF reaction and other foods and products to avoid are further discussed in the red graphic below. A supplement like this one can help counteract accidentally ingesting alcohol or vinegar https://www.amazon.com/dp/B07N32FGK2/ref=cm_sw_r_fa_dp_ZxYiFbQ2QGW4E?fbclid=IwAR3oIsV78p_gmGC-iZr0MZWSw0Hvb4yY5R3KzllYQEJdbI3OOmdCemicwos. It may be something to consider having on hand before starting DSF. Not medical advice, check with your doctor.
HERXHEIMER REACTIONS: My go-to for dizziness is Meclizine/Antivert or Bonine. I start at 25mg and can take more if that’s not enough. For nausea, my go-to is Zofran Rx. Alka Seltzer Gold (ASG) or Tri Salts is great for herxing to alkalize. Both detox bath and ASG or tri salts are used to lower acidity ph and lessen a herx.
PAIN: I use Arnica pellets and arnica topical cream, it's homeopathic and works instantly! It doesn't last as long as medications, but my body has no processing so it's easy and I don't mind taking it multiple times when needed. THE most effective go-to for pain is a detox bath! I was soaking an hour each time up to 3 times a day on bad days. This works best for any Lyme treatment but follows the process in the YouTube link https://www.youtube.com/channel/UCWIlIK3C-J52644PKblX8hw for best results.
G.I. ISSUES: Constipation has been an issue for some. Colonics, enemas, psyllium husk, etc. may be incorporated as needed. If nothing will work, start a new routine of standing on a vibration plate. Using a handheld vibrator otherwise to the belly in a circular motion in the cycle of digestion very gently may help. Include the thighs to increase the chances of a bowel movement. MORE water can help to provide you're not over-hydrating. Diarrhea can happen to others and boiling celery water and drinking it warm can stop it. Also, the use of charcoal or GI Detox binders will help. You may find relief from ridding your diet of roughage, fried, and or spicy foods during the discomfort. Ridding your diet of known allergens may also help like gluten, dairy, corn, soy, and peanuts among others.
DEPRESSION: can happen and we have to remind ourselves to include humor in our daily lives to offset what might be happening in the brain. As an example, I prerecord my favorite night show to watch on my own schedule. Be patient with yourself while you go through this therapy, like any Lyme treatment it will produce die off and your body will be under additional stress. You can search the FB groups for what's worked for others and find supplements to help the dopamine. We are now seeing that people do better avoiding depression by titrating down when ceasing DSF therapy. It has been "suggested" by a retired pharmacist, Cozette Moysa when someone wants to cease DSF therapy, to decrease the first dose you want to start titrating down by 25%. If your core dose is 250 then you'd decrease to 187.5 for 2 weeks and see how you feel. If you do not get an onset of depression and feel okay, decrease another 25% for another 2 weeks. If you do feel depressed, you might consider staying there a while longer. She said this titration should be a slow process and individual, possibly taking about 6 weeks. The first decrease will be the highest amount. ALWAYS talk to your doctor about your medication decisions but as you well know, the studies have not yet been published on how to dose this drug so is our best guess figuring this out together. Your doctor knows your case best, so talk to them about changes. SSRI medication to ease your way down may help. Going off cold turkey can cause a drop in dopamine that can cause some uncomfortable depression. Be careful of this potential and plan ahead to go low and slow to prevent having to come off it quickly. True psychosis is rare and most patients that we've watched in our Facebook forums reporting this feel severe depression from going too high too fast and then herx and have to stop therapy abruptly that can cause a drop in dopamine that can cause debilitating depression. This is avoidable in most cases by planning ahead to go low and slow.
More from retired pharmacist Cozette Moysa, "as with any medication that has the potential to affect mood, the patient response is individual and is therefore unpredictable. Dose titration is frequently done with antidepressants and also, anxiolytics (anti-anxiety medications), also. The brain just doesn’t respond very quickly and easily to medications that affect the smoke of the neurotransmitters.
This is partly because of the neuron's manufacturer and stores them inside. It just takes a while for this process to readjust to whatever was going on before. This is referred to as ’ up-regulation’ and downregulation.’ With antipsychotics, which block dopamine, the need for titrations up or down doesn’t seem to be so necessary. So, disulfiram seeming to need a more regulated approach makes a person wonder if the drug affects more than just dopamine. Maybe it’s the subsequent decrease in norepinephrine, who knows. But these neurotransmitters have an interplay because they are often made with the name neuron. Alcoholics may not have been reported to experience depression post-treatment with disulfiram, but that could be partly explained by the fact that many will stop taking disulfiram and then hit the bottle again, and alcohol is a CNS depressant. If a person becomes drunk, the feelings of depression may become much less noticeable. So, it may not be Lyme patients that are more prone to experiencing temporary depression upon stopping the drug. This effect may just be the drug, itself. It is not addicting or habituation, but disulfiram does affect norepinephrine and dopamine, so it’s only logical that there may be changes that are noticeable. Also, once a medication or treatment is withdrawn, it is not uncommon for discontinuing he treatment to be perceived as a ‘loss’, in the form of it providing a sense of security, even when there are side effects. Kind of like giving up one’s grip on the window sill to climb onto the ladder to escape the burning building.
There may be a period of anxious waiting—either to start feeling better or waiting to see if the Lyme symptoms return. This waiting period is difficult and anxiety-promoting for some people. This is normal. The other thing is—if this medicine is successful, it can take months to feel good again, even after having acute Lyme disease. This is why even IDSA put the diagnosis of PTLDS off-limits until 6 months after treatment is stopped. So, it takes time for the brain to readjust and it is not surprising that some people feel depressed and anxious after taking disulfiram for months. If these feelings go on more than 6-8 weeks or are so very uncomfortable, it might be a temporary job for a psychiatrist. There are no medals given for suffering from depression. Prolonged anxiety often goes along with depression, or precedes depression. Lyme patients also may be suffering from Complex PTSD, so that maybe something that needs attention. Even if treatment is successful, it will still be a change and change can be difficult and scary. All this is something that can be helped by mental health professionals, including psychologists. Therapy combined with medications (when medications are necessary) is the best combination. If needed, utilize these services. I have seen lives completely turned around when people find good professionals who know what they are doing."
DOSING:
“Easy Does It!”, reminds Dr. Liegner.
My favorite saying from Dr. Liegner is, “dose and duration matter”, however, this is still needing studies to show what dose and for how long. His most recent lecture at the September 2020 ILADS virtual conference, he stated the ideal dose is 4mg/kg of body weight to reach lasting remission. Learning how to do this protocol will help you stress less and just plan to be organized ahead of starting DSF. He has helped lead this frontier and has had the longest time working with patients on DSF since 2017. Dr. Kenneth Liegner writes, "Disulfiram is not necessarily a 'walk in the park' and can be trying, so medical guidance with one's treating practitioner is necessary and desirable. As far as 'target' dose when aiming to try to achieve a 'remission' if that is possible, I've come to this very rough 'guestimate' with the goal of using the minimum 'necessary' dosages:
100 lbs or less 250 mg; (101)-150 lbs. 375 mg; 200 lbs. 500 mg. > 200 lbs.,? 750 mg 300 lbs? 1 gram? Recommend close working relationships with ones treating physician. I think practitioners & patients need to work (dosing) out on an individual basis; these days, however, I’m tending to start out @ 125 mg (Every) 3 days for a while. This is potent ‘stuff’ & some have a significant ‘burden of infection’.......so they say, (I think, in AA): Easy Does It!"
Disulfiram In The Treatment Of Lyme & Babesiosis - Retrospective Review Of First 3 Years' Experience In One Medical Practice
Kenneth B Liegner, MD BACKGROUND
High throughput screening found disulfiram more potent versus Bb than conventionally recommended antibiotics in vitro(1). This prompted off-label use of this agent as previously reported (2).
AIMS:
We report our subsequent experience with disulfiram between 3-15-2017 and 3-15-2020. https://www.ilads.org/ilads-conference/ilads-annual-conference-2020/abstract/#disulfiram-in-the-treatment
PATIENTS & METHODS:
Patients were evaluated in the ordinary course of clinical care. In addition to standard treatment methods disulfiram was mentioned as a possible option for the treatment of Lyme disease. For those preferring disulfiram, full discussion was held regarding potential risks, potential benefits and considerable uncertainties with novel application of this agent. 4 of 71 patients were 'lost to follow-up' resulting in 67 evaluable patients.
RESULTS:
Of 67 evaluable patients:
13 of 33 patients (39%) who completed one or two courses of high-dose disulfiram (> or = 4 mg/kg/day) were able to enjoy 'enduring remission' defined as remaining clinically well for > or = 6 months without further anti-infective treatment.
62 of 67 patients (92.5%) endorsed net benefit from the received course or courses of disulfiram, combining the low dose group (<4mg/kg/day), the high dose group and the 'cross-over' group.
5 of 67 patients (7.5%) reported either no benefit or unclear benefit from application of disulfiram
It is unclear whether a low dose regimen can yield 'enduring remission' after discontinuation of treatment
10 of 67 patients (15%) reported development of paresthesias thought consistent with disulfiram-induced peripheral neuropathy. These symptoms completely or substantially resolved over weeks to months with only minimal if any residua in 7 of 10. Mild to moderate residual persisted in 3 of 10.
21 of 67 patients (31%) exhibited emotional instability ranging from hypomania to anxiety and/or depression. Mood disturbance resolved within days to weeks in all patients with cessation of disulfiram although a few required psychiatric intervention.
10 of 67 patients (15%) exhibited mild to moderate hepatic transaminitis which required cessation of treatment in 2 patients. Transaminitis fully resolved in all cases.
CONCLUSIONS:
Disulfiram monotherapy is useful in the treatment of Lyme disease. Regular laboratory monitoring and close clinical follow-up is necessary. Dosages of 4-5 mg/kg/day for 6-12 weeks appear to be optimal for attempting to achieve 'enduring remission' while minimizing adverse effects. Dosages as low as 0.06 - 2 mg/kg/day for indeterminate durations also conferred benefit with minimal adverse effects. An individualized and flexible approach with shared decision-making is particularly suitable in the use of this agent.
"It is a dance", Dr. Dan Kinderlehrer.
Watch this video before starting disulfiram. Dr. Kinderlehrer starts his patients out between 15mg to 125. "It is a dance," he says, so go slow and be safe! https://youtu.be/q6dLPVbUXRQ
Dr. Kinderlehrers dosing follows and is subject to change as time proves what may work better for each individual.
This is for below a 150 lb person based on TOLERABILITY: starting dose can go lower for more sensitive patients.
-1st week 62.5 or 125mg, every third day for the first few weeks. Don't move on if your herxes are unmanageable. If they are not tolerable, get off it and work on detoxing.
Move up every 14 days if u feel okay. Never move up on your dose within 2 weeks as this is how long the drug metabolites remain in your system.
-3rd week 125mg+62.50 (per day)
-5th week 125mg+2x62.50
-7th week 125mg+3x62.50
-9th week 125mg+4x62.50
DIVIDING DOSES: DSF's half-life is 7 hours +/- 1-2 hours. An example on how to take DSF to limit side effects is if I am at 375 mg daily, dividing doses up throughout the day 3 times of 125 mg. My times are dependent on what works that day but usually, it's 7am, 3pm and 10pm. I set a calendar item to repeat to help me remember. Taking them close to 7-8 intervals helps to keep the drug from unstable blood levels per Cozette Moysa, where you get the high peaks and the low troughs. This is suspected to cause the discomfort that we patients feel is a herx or side effect and it is not per a very trusted microbiologist and pharmacologist. If you are just starting out and taking 125 every few days then the same thing, break up your dose 3 ways and take it at 7, 3, and 10pm. Increase if herx is manageable, or take a break if herx is active or extreme until it resolves. Stopping abruptly due to a herx is not recommended to avoid a drop in dopamine if at all possible. Not medical advice and always discuss this with your Dr. Labs for liver and CBC every few weeks.
TAPERING OFF
It's important to not stop cold turkey if you can to avoid jolting the brain. Once symptoms have ceased after Dr. Liegner's suggested 6-12 weeks at core dose, you might talk to your Dr about tapering off the same way you increased dosing slowly when you started. Treating physicians have seen less side effects with dopamine and depression by tapering off. This may take 4- 8 weeks to do. The first adjustment would be the most significant for the brain to adjust to, so see how you do. If depression sets in, you might talk to your doctor about going back up a bit then tapering at a lesser rate. Here is an example and not medical advice:
If you're on 250mg, lowering by 25% would be 187.5 for 2 weeks. Next would be to decrease by 32.25 or 62.5= 125. for 2 weeks then keep lowering by 32.25 or 62.5 every 2-3 weeks if you feel okay. Stopping altogether can be a jolt to the brain and cause depression. Treating with DSF just under a herx is ideal throughout this therapy. A psychiatrist may need to be brought on board if depression starts. We have seen some luck with SSNRI's to adjust the norepinephrine. Anxiety may also become an issue and something like lorazepam has helped some patients. We never recommend a patient to self medicate and to contact their doctor immediately if they have intrusive thoughts. Dr. Robert Bransfield has helped some patients through a "brain herx" with Benadryl and alka seltzer gold. I have heard feedback from patients with head pressure/Lyme encephalitis like symptoms that this WORKS great. Some have also incorporated the detox bath protocol on my YouTube page. It's not just any old bath, there is a process to follow to maximize the benefits.
STINKY? You may notice u begin smelling like sulfur that's not pleasant. I keep essential oils in my purse to help but it's breath and body.. It is the carbon disulfide that produces the smell and won't start until you reach a higher dose nor will it end until you finish the protocol. Just be aware to not breathe too close to people or stand too closely for this short time period. It will go away but there's not much you can do about it!
After my 8-month treatment, I started getting 1-2 IV’s every week to help my energy level. I am doing a 1000ml lactated ringer for the electrolytes and Meyers cocktail. I make a big jug of hot nettle tea daily to help my kidneys. I am working on mitochondria health with Astanxthem and Mitocore multivitamin. There has been information about potential damage to mitochondria on DSF but we won't know until proper studies are continued as it was an initial study that was never followed up on further to be conclusive. I have increased antioxidants during recovery and it took me about 6 months to start feeling better. Some notice marked improvements on this protocol during treatment and some not for months or weeks after cessation. Coffee enema’s/colonics have helped my liver detox. I do one the day after an IV to move out the toxins.
COSTS: With insurance is $10.00 A MONTH but will vary depending on your plan. Cozette Moysa put this out in our DSF group, "cash pay is about $180 for #180 tablets. It has been generic for a very long time. In today’s prices, it is cheap. There is little money to be made on it. It shows promise, but more research on it is needed. For one, they have not determined its mechanism of action. That is important. It passes the blood-brain barrier and is well distributed throughout the body. It kills Bb persisters. It has been reported to work intracellularly. There is no single antibiotic that meets all these requirements. It must be monitored closely and, as with all prescription drugs, there are always potential risks and benefits. The liver problem is thought to be a drug hypersensitivity issue, sort of an allergic-type of response. This happens with other medications, also.
Some preliminary information for those who are curious about disulfiram:
Multiple individual trials of disulfiram in many places, both in the US and abroad, have been going on since last year. I, Cozette Moysa had taken some literature to our daughter’s doctor last year and she was immediately started on it, last September. Other patients were quickly added. Since then, I have compiled information regarding its use in treating alcoholism. A draft of this was distributed on a limited basis to those who were interested. Since its efficacy in humans was unknown, we refrained from making any big announcements.
Based on Lyme disease patient reactions, the drug appears to exert an effect on Borrelia. It’s used in treating Lyme and other tick-borne diseases, however, is off-label is being studied. Reactions and tolerability appear to be individualized. The one piece of information that quickly emerged—dosing must start low and increases must be very slow. The time to reach steady-state blood levels of the two major active metabolites (for ALDH Inhibition) is TWO WEEKS. The mechanism of action in killing Borrelia is unknown. There are several potential actions that disulfiram has against Borrelia. It is a heavy metal chelator, interferes with the Mn-Superoxide Dismutase system, and also inhibits lactate dehydrogenase (not the same as ALDH, which is involved in the breakdown of ethyl alcohol.) These enzymes are present in Borrelia burgdorferi. Then again, there may be another enzyme system that is involved. Research is needed on the mechanism of action. This knowledge may open up new avenues to attack the bacteria, other than using antibiotics to attack the cell wall.
Its distribution is excellent and it passes the blood-brain barrier, which is often an impediment with many antibiotics. I have read that it can act intracellularly but have not seen the proof. The concentration needed to kill or prevent exposed Borrelia from replicating is low (a good thing.)
It can probably penetrate biofilm, but that has not been proven. Also, it kills persister cells, which is likely to be a requirement for late-stage infections. The information is encouraging.
The effective dose is unknown and the duration of therapy is also unknown. Based on results reported by Liegner, a 6-week duration of therapy at the target dose may be insufficient. Further research is needed to determine more information.
It must be stressed—the course of therapy can be rough on some people. It is a long-standing old drug with decades of reports and is reported to have a low-to-moderate side effect profile, But, Lyme patients have reported side effects that can be quite pronounced and uncomfortable, causing them to stop therapy for a while (postulated to be the result of die-off.) Side effects reported in the past (in alcoholics) have been reported to be related to the dose and to the amount of time the patient has been taking disulfiram. So, caution must be exercised to not proceed too quickly. The effects of the drug can take you by surprise, so ‘low and slow’ is being advised. There ARE potential side effects and even some rare but serious adverse effects, including a potentially fatal drug hypersensitivity reaction. As with any prescription medication, patient counseling and careful medical monitoring are both, a must. every few weeks is a suggestion.
Glutathione is okay as we know right now on DSF. Studies need to be done to confirm this. Disulfiram has several identified actions that potentially could contribute to its actions against various bacteria, but the mechanisms may be different, from one bacteria to the other. Personally, I would avoid as many compounds as possible, to keep things as simple as possible. This just makes it easier to figure out, what is causing...what reaction. None of this is medical advice, but is a reporting of what I have been told:
Some of the reactions of Lyme patients have reported may be unique to the pre-existing condition of having inflammation in the brain.
I have been informed there is a somewhat complicated mechanism of transporting disulfiram that is involved with the symptoms of toxicity. Too high of a dose at one time can cause unwanted side effects because of increased uptake of the disulfiram-copper complex that occurs when the oral dose is increased. (Sorry, there are no published references available.)
The spacing out of smaller doses (as opposed to dosing every 24 hours) can help to avoid spikes in the disulfiram-copper complex formed in the stomach blood being carried into the circulation, which can result in more copper being carried into the brain and causing more inflammation. I was told that copper can be more irritating (causing increased inflammation) to an already-inflamed brain secondary to persistent Lyme, as compared to a person with an intact brain. Hence, the increased reports of adverse effects for Lyme patients.
So, the response of a ‘bad reaction’ (that is not usually experienced when Lyme is not present) in the brain is not necessarily a sign the medication is ‘working better.’ It may be more of an indicator there is inflammation there (we know that, already.)
The transporting of higher amounts of copper that do not produce this response in non-Lyme patients —is just causing irritation that does not necessarily provide any additional benefit. Causing more inflammation in the brain is not recommended, so ‘more’ is not necessarily ‘better’ and the speed of getting up to the (unestablished) recommended dose may not be the first issue.
I was told the goal should be to stay within the ‘therapeutic window’ (still, officially not established and accepted.) Human studies will eventually supply that information. The lack of interest in this treatment has created a situation where treating physicians and patients are left to their own devices, again. Based on this information, it can be THEORIZED that the determination of disulfiram dosing must FIRST be determined by what is tolerable to the individual patient. So, the dose must be individualized between the doctor and patient (as always.) There appears to be, AT THIS TIME, no one-size-fits-all dosing algorithm. Treating Lyme with disulfiram is a novel use of this medication and nothing has been officially established, yet. The lack of information caused by insufficient and flawed research for the past (almost) 30 years has created this situation, where patients and their doctors have been left with making the decision of conducted ‘trial-by-error’ therapy, vs. ‘doing nothing’ therapy. Disulfiram is showing promise. So far, the adage of ‘low and slow’ and the concept of individualized therapy is thought to be the best course of action. Ultimately, the choice of medication, after weighing the benefits vs, risks, and the dosing must be worked out between the patient and their doctorCoco Lake: Disulfiram kills both active and dormant persisters. It is one reason that makes it so different from the antibiotics recommended by IDSA. They ALL failed the lab tests done on mature cultures. Only 4 successive rounds of ceftriaxone worked in the lab. (It’s a lot more challenging to kill Borrelia in the body.)
PERSISTERS: Borrelia does not have the genes to develop resistance to antibiotics. DSF is not an antibiotic, but the lack of those genes suggests it has never acquired the ability to make the changes needed (didn’t need to) to develop a new compensatory mechanism to outsmart disulfiram. It is probably the persister bacteria (which love to hang out in biofilm) that are able to hide until an antibiotic is stopped. They revert to active replicating cells after about 14 days and reach their peak at around 21 days. Since they love to hide inside biofilm and also, in sites where antibiotics don’t reach very well, they are able to stay safe, until whatever antibiotics are thrown at them—are stopped. Eventually, they return and start replicating, and—the infection returns. Disulfiram attacks the active spirochetes AND the persisters. The drug is widely distributed throughout the body and the CNS. Biofilm has not been reported to be a problem. The problem is the side effects/toxicity, due mainly to its metabolism, along with the inhibition of alcohol metabolism. And also, it is a potent killer of Borrelia. Lyme patients have inflammation and disulfiram’s actions can increase inflammation."
Look for drug interactions here:
https://www.drugs.com/drug-interactions/disulfiram.html
Liver Function Tests (LFT’s):
Liver function tests are a set of blood tests commonly done to check on the health of your liver. Changes in liver function tests give a clue as to whether your liver is under strain, inflamed, infected or diseased, and how badly. The pattern of the tests can give a clue to the cause and can allow early detection of unsuspected problems, and monitoring of known problems. These are the 'surveillance' labs Dr. Liegner orders his patients- CBC w. diff; BUN & creatinine; AST, ALT, GGT, T. bili.; CPK & urinalysis (*e.g. U/A). Probably good idea to do it Q 2 weeks for first month, thereafter, monthly probably OK unless derangements seen. SCHEDULE: Before starting DSF then every 2 weeks for the first few months on DSF. https://patient.info/digestive-health/abnormal-liver-function-tests-leaflet?fbclid=IwAR3iP6eIT8C7sioShBm-X2Eytwe4qeUgJaaHprjqV6Xu6k27SrHeLA6pOBo#nav-6
More information from Dr. Liegner is in the video on Kristina's YouTube channel with Dr. Liegner and Dr. Rajadas found here: https://youtu.be/KtmLxaA8stU.
Join our public page for the latest disulfiram information at “Disulfiram for Lyme”, and for private discussion at “Disulfiram Experience for Lyme Support Group”. We are all in this together and willing to help you. As time allows, I offer mentorship in the Support Group. I hope that medical professional and others who continue to get through this treatment offer to coach and join our group in mentoring patients. Nothing discussed is medical advice, only support from experience is offered. Try to share how you’re doing or ask questions; we all try to help as we can.
Updated 12/13/2020, do not copy or share without crediting Kristina Bauer and those who provided information above. This is for informational and educational purposes only and not to be used in place of medical advice from your treating physician.
Other foods known to cause problems on DSF is green tea, polyphenols and cistus tea. Anything fermented like parmesan cheese is a likely suspect for causing a DSF reaction that surprised us. Some do fine, others don't.
Thinking about taking or prescribing disulfiram for Lyme & coinfections?
Read here and prepare FIRST for the safest and best outcome using this very effective medication!
What it treats:
Disulfiram has shown to be effective treating and or eradicating borrelia and babesiosis, aspergillus mold, vermicide, and possibly virus's per the HIV study. What studies we have are below to support this. Some patients report their bartonella symptoms can flare while on DSF, but how effectively it's killing it is yet to be known. None of this website or page is medical advice and for informational purposes only. This reference guide was made from what expert doctors with the most experience studying, publishing and using the drug have shared in treating persistent Lyme and coinfections with disulfiram (DSF). Talk to your treating physician about the use of any medication and check for drug interactions prior to starting including any THC or CBC products. All links are shared below for an all-encompassing reference guide to date.
“The tortoise will always beat the hare”, Dr. Daniel Kinderlehrer.
If you are sensitive to treatments, you can start prior to disulfiram by prepping the body for treatment. Incorporating a binder and detox protocol 2-3 x's a day is important to help the body flush the lymph and organs before we increase the load of die-off. Stay hydrated! Drink 2 oz of water every 15 minutes is a nice reminder to stay hydrated and free of constipation. Our brains love hydration too and you will have more energy and generally feel better. Binders are products that pull toxins from the body like activated charcoal, bentonite clay, cholestyramine, Enterosgel and G.I. Detox are some patient favorites. Take this away from food and supplements or medication at least an hour.
A good detox protocol might include infrared saunas (low EMF) a few days a week opposite to days you might do colonics/enemas. There are many ways to detox but some typical ways Lyme patients have benefited have been by the use of dual ionic foot baths, saunas, liver support, and juicing. Liver support might include milk thistle, ALA, glutathione, NAC, and coffee enemas. We want to support the liver to improve its function and efficiency. Liver damage is a rare side effect on DSF, but Lyme patients need to increase supporting the organs doing the most work ie, liver, gallbladder, and kidneys. Consider adding light rebounding if you’re able, to help lymph get moving; arms above the head for the best approach.
Any mold and candida treatment or heavy metal toxicity should be considered before DSF treatment. Test to check if these are at higher than normal levels and work the protocols to get them to a healthy level. It's also a good idea to ask your Dr. to check you for how high your histamine and cortisol levels are and treat you appropriately prior to adding DSF therapy that may increase die off, thus increasing inflammation and cytokine production. Antioxidants can be of help during DSF treatment but needs studied further. Supplements can contain metals that may bind with DSF and should be avoided.
Those can include:
Silver
Copper
Iron
Here's a link to Kristina's dedicated channel on Lyme for information about detox baths and other modalities to help you heal https://www.youtube.com/channel/UCWIlIK3C-J52644PKblX8hw. Detox baths are an inexpensive way to alkalize the body and lessen pain. Patients report this has been very effective for anything from fibromyalgia to brain swelling and migraines. Refrain from apple cider vinegar in your bath as it can react while on DSF. This varies per person. Any sauna work will INCREASE die off as it forces a fever. Some days maybe binders or Burbur/Pinella (Nutramedix.com) may be a better approach if you’re already experiencing a herx. We want to lessen that burden while treating tick-borne illness, not increase it. Another helpful tool would be to consider colonics or coffee enemas.
As to Dr. Kinderlehrer’s reference above, going slow on this protocol like a tortoise will always beat the hare who goes fast and hard. Patients tend to experience fewer toxic feelings of side effects and herxing working this approach he suggests.
A few things to consider. Oxidative therapies like hBot and ozone can increase die off and cause herxing. We want to focus on one intervention at a time and refrain from increasing inflammation, treating with DSF just under a herx to avoid producing more histamine that can build upon the next dose. A good diet on DSF will vary depending on your sensitivities but thinking in terms of eating “whole foods” might help. Foods to avoid while on disulfiram is any alcoholic beverage, anything fermented like kombucha, rice, yeast and possibly even, probiotics. Ketchup, dressing, mustard and some soy sauce has vinegar, shampoo and lotions have alcohol. Some people are sensitive and react to rubbing alcohol when giving blood while others don’t at all. It’s best to not chance it but is an individual.
ACETALDEHYDE: Some vaping mixtures contain alcohol and should be avoided. Herbal tinctures, some stevia, vanilla extract, and homeopathy also sometimes contain alcohol. Check everything first in your kitchen and bathroom and eliminate your risk prior to starting your treatment. It will be easier to be successful when well-planned beforehand. Avoid any mentholated topical essential oils such as menthol, peppermint, and spearmint. Anything that ends in "ol" can contain alcohol like thiols. Overly ripe fruit can cause a DSF reaction and other foods and products to avoid are further discussed in the red graphic below. A supplement like this one can help counteract accidentally ingesting alcohol or vinegar https://www.amazon.com/dp/B07N32FGK2/ref=cm_sw_r_fa_dp_ZxYiFbQ2QGW4E?fbclid=IwAR3oIsV78p_gmGC-iZr0MZWSw0Hvb4yY5R3KzllYQEJdbI3OOmdCemicwos. It may be something to consider having on hand before starting DSF. Not medical advice, check with your doctor.
HERXHEIMER REACTIONS: My go-to for dizziness is Meclizine/Antivert or Bonine. I start at 25mg and can take more if that’s not enough. For nausea, my go-to is Zofran Rx. Alka Seltzer Gold (ASG) or Tri Salts is great for herxing to alkalize. Both detox bath and ASG or tri salts are used to lower acidity ph and lessen a herx.
PAIN: I use Arnica pellets and arnica topical cream, it's homeopathic and works instantly! It doesn't last as long as medications, but my body has no processing so it's easy and I don't mind taking it multiple times when needed. THE most effective go-to for pain is a detox bath! I was soaking an hour each time up to 3 times a day on bad days. This works best for any Lyme treatment but follows the process in the YouTube link https://www.youtube.com/channel/UCWIlIK3C-J52644PKblX8hw for best results.
G.I. ISSUES: Constipation has been an issue for some. Colonics, enemas, psyllium husk, etc. may be incorporated as needed. If nothing will work, start a new routine of standing on a vibration plate. Using a handheld vibrator otherwise to the belly in a circular motion in the cycle of digestion very gently may help. Include the thighs to increase the chances of a bowel movement. MORE water can help to provide you're not over-hydrating. Diarrhea can happen to others and boiling celery water and drinking it warm can stop it. Also, the use of charcoal or GI Detox binders will help. You may find relief from ridding your diet of roughage, fried, and or spicy foods during the discomfort. Ridding your diet of known allergens may also help like gluten, dairy, corn, soy, and peanuts among others.
DEPRESSION: can happen and we have to remind ourselves to include humor in our daily lives to offset what might be happening in the brain. As an example, I prerecord my favorite night show to watch on my own schedule. Be patient with yourself while you go through this therapy, like any Lyme treatment it will produce die off and your body will be under additional stress. You can search the FB groups for what's worked for others and find supplements to help the dopamine. We are now seeing that people do better avoiding depression by titrating down when ceasing DSF therapy. It has been "suggested" by a retired pharmacist, Cozette Moysa when someone wants to cease DSF therapy, to decrease the first dose you want to start titrating down by 25%. If your core dose is 250 then you'd decrease to 187.5 for 2 weeks and see how you feel. If you do not get an onset of depression and feel okay, decrease another 25% for another 2 weeks. If you do feel depressed, you might consider staying there a while longer. She said this titration should be a slow process and individual, possibly taking about 6 weeks. The first decrease will be the highest amount. ALWAYS talk to your doctor about your medication decisions but as you well know, the studies have not yet been published on how to dose this drug so is our best guess figuring this out together. Your doctor knows your case best, so talk to them about changes. SSRI medication to ease your way down may help. Going off cold turkey can cause a drop in dopamine that can cause some uncomfortable depression. Be careful of this potential and plan ahead to go low and slow to prevent having to come off it quickly. True psychosis is rare and most patients that we've watched in our Facebook forums reporting this feel severe depression from going too high too fast and then herx and have to stop therapy abruptly that can cause a drop in dopamine that can cause debilitating depression. This is avoidable in most cases by planning ahead to go low and slow.
More from retired pharmacist Cozette Moysa, "as with any medication that has the potential to affect mood, the patient response is individual and is therefore unpredictable. Dose titration is frequently done with antidepressants and also, anxiolytics (anti-anxiety medications), also. The brain just doesn’t respond very quickly and easily to medications that affect the smoke of the neurotransmitters.
This is partly because of the neuron's manufacturer and stores them inside. It just takes a while for this process to readjust to whatever was going on before. This is referred to as ’ up-regulation’ and downregulation.’ With antipsychotics, which block dopamine, the need for titrations up or down doesn’t seem to be so necessary. So, disulfiram seeming to need a more regulated approach makes a person wonder if the drug affects more than just dopamine. Maybe it’s the subsequent decrease in norepinephrine, who knows. But these neurotransmitters have an interplay because they are often made with the name neuron. Alcoholics may not have been reported to experience depression post-treatment with disulfiram, but that could be partly explained by the fact that many will stop taking disulfiram and then hit the bottle again, and alcohol is a CNS depressant. If a person becomes drunk, the feelings of depression may become much less noticeable. So, it may not be Lyme patients that are more prone to experiencing temporary depression upon stopping the drug. This effect may just be the drug, itself. It is not addicting or habituation, but disulfiram does affect norepinephrine and dopamine, so it’s only logical that there may be changes that are noticeable. Also, once a medication or treatment is withdrawn, it is not uncommon for discontinuing he treatment to be perceived as a ‘loss’, in the form of it providing a sense of security, even when there are side effects. Kind of like giving up one’s grip on the window sill to climb onto the ladder to escape the burning building.
There may be a period of anxious waiting—either to start feeling better or waiting to see if the Lyme symptoms return. This waiting period is difficult and anxiety-promoting for some people. This is normal. The other thing is—if this medicine is successful, it can take months to feel good again, even after having acute Lyme disease. This is why even IDSA put the diagnosis of PTLDS off-limits until 6 months after treatment is stopped. So, it takes time for the brain to readjust and it is not surprising that some people feel depressed and anxious after taking disulfiram for months. If these feelings go on more than 6-8 weeks or are so very uncomfortable, it might be a temporary job for a psychiatrist. There are no medals given for suffering from depression. Prolonged anxiety often goes along with depression, or precedes depression. Lyme patients also may be suffering from Complex PTSD, so that maybe something that needs attention. Even if treatment is successful, it will still be a change and change can be difficult and scary. All this is something that can be helped by mental health professionals, including psychologists. Therapy combined with medications (when medications are necessary) is the best combination. If needed, utilize these services. I have seen lives completely turned around when people find good professionals who know what they are doing."
DOSING:
“Easy Does It!”, reminds Dr. Liegner.
My favorite saying from Dr. Liegner is, “dose and duration matter”, however, this is still needing studies to show what dose and for how long. His most recent lecture at the September 2020 ILADS virtual conference, he stated the ideal dose is 4mg/kg of body weight to reach lasting remission. Learning how to do this protocol will help you stress less and just plan to be organized ahead of starting DSF. He has helped lead this frontier and has had the longest time working with patients on DSF since 2017. Dr. Kenneth Liegner writes, "Disulfiram is not necessarily a 'walk in the park' and can be trying, so medical guidance with one's treating practitioner is necessary and desirable. As far as 'target' dose when aiming to try to achieve a 'remission' if that is possible, I've come to this very rough 'guestimate' with the goal of using the minimum 'necessary' dosages:
100 lbs or less 250 mg; (101)-150 lbs. 375 mg; 200 lbs. 500 mg. > 200 lbs.,? 750 mg 300 lbs? 1 gram? Recommend close working relationships with ones treating physician. I think practitioners & patients need to work (dosing) out on an individual basis; these days, however, I’m tending to start out @ 125 mg (Every) 3 days for a while. This is potent ‘stuff’ & some have a significant ‘burden of infection’.......so they say, (I think, in AA): Easy Does It!"
Disulfiram In The Treatment Of Lyme & Babesiosis - Retrospective Review Of First 3 Years' Experience In One Medical Practice
Kenneth B Liegner, MD BACKGROUND
High throughput screening found disulfiram more potent versus Bb than conventionally recommended antibiotics in vitro(1). This prompted off-label use of this agent as previously reported (2).
AIMS:
We report our subsequent experience with disulfiram between 3-15-2017 and 3-15-2020. https://www.ilads.org/ilads-conference/ilads-annual-conference-2020/abstract/#disulfiram-in-the-treatment
PATIENTS & METHODS:
Patients were evaluated in the ordinary course of clinical care. In addition to standard treatment methods disulfiram was mentioned as a possible option for the treatment of Lyme disease. For those preferring disulfiram, full discussion was held regarding potential risks, potential benefits and considerable uncertainties with novel application of this agent. 4 of 71 patients were 'lost to follow-up' resulting in 67 evaluable patients.
RESULTS:
Of 67 evaluable patients:
13 of 33 patients (39%) who completed one or two courses of high-dose disulfiram (> or = 4 mg/kg/day) were able to enjoy 'enduring remission' defined as remaining clinically well for > or = 6 months without further anti-infective treatment.
62 of 67 patients (92.5%) endorsed net benefit from the received course or courses of disulfiram, combining the low dose group (<4mg/kg/day), the high dose group and the 'cross-over' group.
5 of 67 patients (7.5%) reported either no benefit or unclear benefit from application of disulfiram
It is unclear whether a low dose regimen can yield 'enduring remission' after discontinuation of treatment
10 of 67 patients (15%) reported development of paresthesias thought consistent with disulfiram-induced peripheral neuropathy. These symptoms completely or substantially resolved over weeks to months with only minimal if any residua in 7 of 10. Mild to moderate residual persisted in 3 of 10.
21 of 67 patients (31%) exhibited emotional instability ranging from hypomania to anxiety and/or depression. Mood disturbance resolved within days to weeks in all patients with cessation of disulfiram although a few required psychiatric intervention.
10 of 67 patients (15%) exhibited mild to moderate hepatic transaminitis which required cessation of treatment in 2 patients. Transaminitis fully resolved in all cases.
CONCLUSIONS:
Disulfiram monotherapy is useful in the treatment of Lyme disease. Regular laboratory monitoring and close clinical follow-up is necessary. Dosages of 4-5 mg/kg/day for 6-12 weeks appear to be optimal for attempting to achieve 'enduring remission' while minimizing adverse effects. Dosages as low as 0.06 - 2 mg/kg/day for indeterminate durations also conferred benefit with minimal adverse effects. An individualized and flexible approach with shared decision-making is particularly suitable in the use of this agent.
"It is a dance", Dr. Dan Kinderlehrer.
Watch this video before starting disulfiram. Dr. Kinderlehrer starts his patients out between 15mg to 125. "It is a dance," he says, so go slow and be safe! https://youtu.be/q6dLPVbUXRQ
Dr. Kinderlehrers dosing follows and is subject to change as time proves what may work better for each individual.
This is for below a 150 lb person based on TOLERABILITY: starting dose can go lower for more sensitive patients.
-1st week 62.5 or 125mg, every third day for the first few weeks. Don't move on if your herxes are unmanageable. If they are not tolerable, get off it and work on detoxing.
Move up every 14 days if u feel okay. Never move up on your dose within 2 weeks as this is how long the drug metabolites remain in your system.
-3rd week 125mg+62.50 (per day)
-5th week 125mg+2x62.50
-7th week 125mg+3x62.50
-9th week 125mg+4x62.50
DIVIDING DOSES: DSF's half-life is 7 hours +/- 1-2 hours. An example on how to take DSF to limit side effects is if I am at 375 mg daily, dividing doses up throughout the day 3 times of 125 mg. My times are dependent on what works that day but usually, it's 7am, 3pm and 10pm. I set a calendar item to repeat to help me remember. Taking them close to 7-8 intervals helps to keep the drug from unstable blood levels per Cozette Moysa, where you get the high peaks and the low troughs. This is suspected to cause the discomfort that we patients feel is a herx or side effect and it is not per a very trusted microbiologist and pharmacologist. If you are just starting out and taking 125 every few days then the same thing, break up your dose 3 ways and take it at 7, 3, and 10pm. Increase if herx is manageable, or take a break if herx is active or extreme until it resolves. Stopping abruptly due to a herx is not recommended to avoid a drop in dopamine if at all possible. Not medical advice and always discuss this with your Dr. Labs for liver and CBC every few weeks.
TAPERING OFF
It's important to not stop cold turkey if you can to avoid jolting the brain. Once symptoms have ceased after Dr. Liegner's suggested 6-12 weeks at core dose, you might talk to your Dr about tapering off the same way you increased dosing slowly when you started. Treating physicians have seen less side effects with dopamine and depression by tapering off. This may take 4- 8 weeks to do. The first adjustment would be the most significant for the brain to adjust to, so see how you do. If depression sets in, you might talk to your doctor about going back up a bit then tapering at a lesser rate. Here is an example and not medical advice:
If you're on 250mg, lowering by 25% would be 187.5 for 2 weeks. Next would be to decrease by 32.25 or 62.5= 125. for 2 weeks then keep lowering by 32.25 or 62.5 every 2-3 weeks if you feel okay. Stopping altogether can be a jolt to the brain and cause depression. Treating with DSF just under a herx is ideal throughout this therapy. A psychiatrist may need to be brought on board if depression starts. We have seen some luck with SSNRI's to adjust the norepinephrine. Anxiety may also become an issue and something like lorazepam has helped some patients. We never recommend a patient to self medicate and to contact their doctor immediately if they have intrusive thoughts. Dr. Robert Bransfield has helped some patients through a "brain herx" with Benadryl and alka seltzer gold. I have heard feedback from patients with head pressure/Lyme encephalitis like symptoms that this WORKS great. Some have also incorporated the detox bath protocol on my YouTube page. It's not just any old bath, there is a process to follow to maximize the benefits.
STINKY? You may notice u begin smelling like sulfur that's not pleasant. I keep essential oils in my purse to help but it's breath and body.. It is the carbon disulfide that produces the smell and won't start until you reach a higher dose nor will it end until you finish the protocol. Just be aware to not breathe too close to people or stand too closely for this short time period. It will go away but there's not much you can do about it!
After my 8-month treatment, I started getting 1-2 IV’s every week to help my energy level. I am doing a 1000ml lactated ringer for the electrolytes and Meyers cocktail. I make a big jug of hot nettle tea daily to help my kidneys. I am working on mitochondria health with Astanxthem and Mitocore multivitamin. There has been information about potential damage to mitochondria on DSF but we won't know until proper studies are continued as it was an initial study that was never followed up on further to be conclusive. I have increased antioxidants during recovery and it took me about 6 months to start feeling better. Some notice marked improvements on this protocol during treatment and some not for months or weeks after cessation. Coffee enema’s/colonics have helped my liver detox. I do one the day after an IV to move out the toxins.
COSTS: With insurance is $10.00 A MONTH but will vary depending on your plan. Cozette Moysa put this out in our DSF group, "cash pay is about $180 for #180 tablets. It has been generic for a very long time. In today’s prices, it is cheap. There is little money to be made on it. It shows promise, but more research on it is needed. For one, they have not determined its mechanism of action. That is important. It passes the blood-brain barrier and is well distributed throughout the body. It kills Bb persisters. It has been reported to work intracellularly. There is no single antibiotic that meets all these requirements. It must be monitored closely and, as with all prescription drugs, there are always potential risks and benefits. The liver problem is thought to be a drug hypersensitivity issue, sort of an allergic-type of response. This happens with other medications, also.
Some preliminary information for those who are curious about disulfiram:
Multiple individual trials of disulfiram in many places, both in the US and abroad, have been going on since last year. I, Cozette Moysa had taken some literature to our daughter’s doctor last year and she was immediately started on it, last September. Other patients were quickly added. Since then, I have compiled information regarding its use in treating alcoholism. A draft of this was distributed on a limited basis to those who were interested. Since its efficacy in humans was unknown, we refrained from making any big announcements.
Based on Lyme disease patient reactions, the drug appears to exert an effect on Borrelia. It’s used in treating Lyme and other tick-borne diseases, however, is off-label is being studied. Reactions and tolerability appear to be individualized. The one piece of information that quickly emerged—dosing must start low and increases must be very slow. The time to reach steady-state blood levels of the two major active metabolites (for ALDH Inhibition) is TWO WEEKS. The mechanism of action in killing Borrelia is unknown. There are several potential actions that disulfiram has against Borrelia. It is a heavy metal chelator, interferes with the Mn-Superoxide Dismutase system, and also inhibits lactate dehydrogenase (not the same as ALDH, which is involved in the breakdown of ethyl alcohol.) These enzymes are present in Borrelia burgdorferi. Then again, there may be another enzyme system that is involved. Research is needed on the mechanism of action. This knowledge may open up new avenues to attack the bacteria, other than using antibiotics to attack the cell wall.
Its distribution is excellent and it passes the blood-brain barrier, which is often an impediment with many antibiotics. I have read that it can act intracellularly but have not seen the proof. The concentration needed to kill or prevent exposed Borrelia from replicating is low (a good thing.)
It can probably penetrate biofilm, but that has not been proven. Also, it kills persister cells, which is likely to be a requirement for late-stage infections. The information is encouraging.
The effective dose is unknown and the duration of therapy is also unknown. Based on results reported by Liegner, a 6-week duration of therapy at the target dose may be insufficient. Further research is needed to determine more information.
It must be stressed—the course of therapy can be rough on some people. It is a long-standing old drug with decades of reports and is reported to have a low-to-moderate side effect profile, But, Lyme patients have reported side effects that can be quite pronounced and uncomfortable, causing them to stop therapy for a while (postulated to be the result of die-off.) Side effects reported in the past (in alcoholics) have been reported to be related to the dose and to the amount of time the patient has been taking disulfiram. So, caution must be exercised to not proceed too quickly. The effects of the drug can take you by surprise, so ‘low and slow’ is being advised. There ARE potential side effects and even some rare but serious adverse effects, including a potentially fatal drug hypersensitivity reaction. As with any prescription medication, patient counseling and careful medical monitoring are both, a must. every few weeks is a suggestion.
Glutathione is okay as we know right now on DSF. Studies need to be done to confirm this. Disulfiram has several identified actions that potentially could contribute to its actions against various bacteria, but the mechanisms may be different, from one bacteria to the other. Personally, I would avoid as many compounds as possible, to keep things as simple as possible. This just makes it easier to figure out, what is causing...what reaction. None of this is medical advice, but is a reporting of what I have been told:
Some of the reactions of Lyme patients have reported may be unique to the pre-existing condition of having inflammation in the brain.
I have been informed there is a somewhat complicated mechanism of transporting disulfiram that is involved with the symptoms of toxicity. Too high of a dose at one time can cause unwanted side effects because of increased uptake of the disulfiram-copper complex that occurs when the oral dose is increased. (Sorry, there are no published references available.)
The spacing out of smaller doses (as opposed to dosing every 24 hours) can help to avoid spikes in the disulfiram-copper complex formed in the stomach blood being carried into the circulation, which can result in more copper being carried into the brain and causing more inflammation. I was told that copper can be more irritating (causing increased inflammation) to an already-inflamed brain secondary to persistent Lyme, as compared to a person with an intact brain. Hence, the increased reports of adverse effects for Lyme patients.
So, the response of a ‘bad reaction’ (that is not usually experienced when Lyme is not present) in the brain is not necessarily a sign the medication is ‘working better.’ It may be more of an indicator there is inflammation there (we know that, already.)
The transporting of higher amounts of copper that do not produce this response in non-Lyme patients —is just causing irritation that does not necessarily provide any additional benefit. Causing more inflammation in the brain is not recommended, so ‘more’ is not necessarily ‘better’ and the speed of getting up to the (unestablished) recommended dose may not be the first issue.
I was told the goal should be to stay within the ‘therapeutic window’ (still, officially not established and accepted.) Human studies will eventually supply that information. The lack of interest in this treatment has created a situation where treating physicians and patients are left to their own devices, again. Based on this information, it can be THEORIZED that the determination of disulfiram dosing must FIRST be determined by what is tolerable to the individual patient. So, the dose must be individualized between the doctor and patient (as always.) There appears to be, AT THIS TIME, no one-size-fits-all dosing algorithm. Treating Lyme with disulfiram is a novel use of this medication and nothing has been officially established, yet. The lack of information caused by insufficient and flawed research for the past (almost) 30 years has created this situation, where patients and their doctors have been left with making the decision of conducted ‘trial-by-error’ therapy, vs. ‘doing nothing’ therapy. Disulfiram is showing promise. So far, the adage of ‘low and slow’ and the concept of individualized therapy is thought to be the best course of action. Ultimately, the choice of medication, after weighing the benefits vs, risks, and the dosing must be worked out between the patient and their doctorCoco Lake: Disulfiram kills both active and dormant persisters. It is one reason that makes it so different from the antibiotics recommended by IDSA. They ALL failed the lab tests done on mature cultures. Only 4 successive rounds of ceftriaxone worked in the lab. (It’s a lot more challenging to kill Borrelia in the body.)
PERSISTERS: Borrelia does not have the genes to develop resistance to antibiotics. DSF is not an antibiotic, but the lack of those genes suggests it has never acquired the ability to make the changes needed (didn’t need to) to develop a new compensatory mechanism to outsmart disulfiram. It is probably the persister bacteria (which love to hang out in biofilm) that are able to hide until an antibiotic is stopped. They revert to active replicating cells after about 14 days and reach their peak at around 21 days. Since they love to hide inside biofilm and also, in sites where antibiotics don’t reach very well, they are able to stay safe, until whatever antibiotics are thrown at them—are stopped. Eventually, they return and start replicating, and—the infection returns. Disulfiram attacks the active spirochetes AND the persisters. The drug is widely distributed throughout the body and the CNS. Biofilm has not been reported to be a problem. The problem is the side effects/toxicity, due mainly to its metabolism, along with the inhibition of alcohol metabolism. And also, it is a potent killer of Borrelia. Lyme patients have inflammation and disulfiram’s actions can increase inflammation."
Look for drug interactions here:
https://www.drugs.com/drug-interactions/disulfiram.html
Liver Function Tests (LFT’s):
Liver function tests are a set of blood tests commonly done to check on the health of your liver. Changes in liver function tests give a clue as to whether your liver is under strain, inflamed, infected or diseased, and how badly. The pattern of the tests can give a clue to the cause and can allow early detection of unsuspected problems, and monitoring of known problems. These are the 'surveillance' labs Dr. Liegner orders his patients- CBC w. diff; BUN & creatinine; AST, ALT, GGT, T. bili.; CPK & urinalysis (*e.g. U/A). Probably good idea to do it Q 2 weeks for first month, thereafter, monthly probably OK unless derangements seen. SCHEDULE: Before starting DSF then every 2 weeks for the first few months on DSF. https://patient.info/digestive-health/abnormal-liver-function-tests-leaflet?fbclid=IwAR3iP6eIT8C7sioShBm-X2Eytwe4qeUgJaaHprjqV6Xu6k27SrHeLA6pOBo#nav-6
More information from Dr. Liegner is in the video on Kristina's YouTube channel with Dr. Liegner and Dr. Rajadas found here: https://youtu.be/KtmLxaA8stU.
Join our public page for the latest disulfiram information at “Disulfiram for Lyme”, and for private discussion at “Disulfiram Experience for Lyme Support Group”. We are all in this together and willing to help you. As time allows, I offer mentorship in the Support Group. I hope that medical professional and others who continue to get through this treatment offer to coach and join our group in mentoring patients. Nothing discussed is medical advice, only support from experience is offered. Try to share how you’re doing or ask questions; we all try to help as we can.
Updated 12/13/2020, do not copy or share without crediting Kristina Bauer and those who provided information above. This is for informational and educational purposes only and not to be used in place of medical advice from your treating physician.
Other foods known to cause problems on DSF is green tea, polyphenols and cistus tea. Anything fermented like parmesan cheese is a likely suspect for causing a DSF reaction that surprised us. Some do fine, others don't.

A patient interviews Dr. Kinderlehrer about disulfiram for Lyme disease. A brief history of Kristina Bauer's struggle included.
https://www.lymedisease.org/bauer-interview-disulfiram/
https://www.lymedisease.org/bauer-interview-disulfiram/

What is disulfiram and why is it sparking excitement in the Lyme community?
Click here to learn all about this off label use for persistent Lyme complex.
https://www.lymedisease.org/disulfiram-bauer-moysa/
Click here to learn all about this off label use for persistent Lyme complex.
https://www.lymedisease.org/disulfiram-bauer-moysa/
Sources for patients and the medical community
Articles on persistent borrelia & Disulfiram 2015 +:
Peer-Reviewed Evidence of Persistence of Lyme Disease Spirochete Borrelia burgdorferi and Tick-
Borne Diseases
The following is a list of over 700 peer-reviewed articles that support the evidence of persistence of Lyme and other tick-borne diseases. It is organized into different categories—general, neuropsychiatric, dementia and congenital transmission.
www.ilads.org/wp-content/uploads/2018/07/CLDList-ILADS.pdf
“Repurposing” Disulfiram in the Treatment of Lyme Disease and Babesiosis:
Retrospective Review of First 3 Years’ Experience in One Medical Practice, Dr. Kenneth Liegner 2020
https://pubmed.ncbi.nlm.nih.gov/33291557/
Studies in Bb persister cells that led to studying disulfiram and the newer in vitro drug studies:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4576077/
https://www.ncbi.nlm.nih.gov/pubmed/26014929
Initial discovery of Disulfiram eradicating Persistent Lyme by Dr. Rajadas and Dr. VR Pothineni:
https://med.stanford.edu/news/all-news/2016/04/new-compounds-have-potential-to-combat-lyme-disease.html
Successful mouse study on Disulfiram for Persistent Lyme by Dr. Rajadas and his BioADD lab at Stanford:
https://www.biorxiv.org/content/10.1101/842286v1?rss=1
Columbia 2019-2021 clinical study on disulfiram:
https://clinicaltrials.gov/ct2/show/NCT03891667
Bay Area Lyme: The Disulfiram Story - by Bonnie Crater:
https://www.bayarealyme.org/blog/in-search-of-a-cure-for-lyme-disease-the-disulfiram-story/
Disulfiram (Tetraethylthiuram Disulfide) in the Treatment of Lyme Disease and Babesiosis: Report of Experience in Three Cases by Dr. Kenneth B. Liegner:
https://www.mdpi.com/2079-6382/8/2/72/htm?fbclid=IwAR2HFnDvVjTIjar4ig_KcDqmxW9OABbWOEeEfp_9MvaS2lWzjeMhHoJXf6I
“It is apparent from these data that B. burgdorferi bacteria, which have had time to adapt to their host, have the ability to escape immune recognition, tolerate the antibiotic doxycycline and invade vital organs such as the brain and heart,” said lead author Monica Embers, PhD, assistant professor of microbiology and immunology at Tulane University School of Medicine.
https://www.lymedisease.org/lyme-study-embers/
An excellent review of the literature on Bb persisters, that led to disulfiram being studied to kill persisters:
https://www.ncbi.nlm.nih.gov/pubmed/31097026
Peer-Reviewed Evidence of Persistence of Lyme Disease Spirochete Borrelia burgdorferi and Tick-Borne Diseases
The following is a list of over 700 peer-reviewed articles that support the evidence of persistence of Lyme and other tick-borne diseases. It is organized into different categories—general, neuropsychiatric, dementia and congenital transmission.
www.ilads.org/wp-content/uploads/2018/07/CLDList-ILADS.pdf
A note from Dr. Liegner on potential risks:
"I think this work is very important to be mindful of. Those of us who prescribe disulfiram and the patients who receive it must be aware of these significant toxicities/risks. It is a bit like cancer chemotherapy: it can help but also can harm. So dosages & durations need to be kept in mind, with vigilance for early detection of toxicities and cessation of the drug. Dr. Valentine's 'body of work' on disulfiram is very prodigious and insightful."
Here's the associated files to help educate you on the need for caution in using DSF as a treatment for Lyme and coinfections:
Articles on persistent borrelia & Disulfiram 2015 +:
Peer-Reviewed Evidence of Persistence of Lyme Disease Spirochete Borrelia burgdorferi and Tick-
Borne Diseases
The following is a list of over 700 peer-reviewed articles that support the evidence of persistence of Lyme and other tick-borne diseases. It is organized into different categories—general, neuropsychiatric, dementia and congenital transmission.
www.ilads.org/wp-content/uploads/2018/07/CLDList-ILADS.pdf
“Repurposing” Disulfiram in the Treatment of Lyme Disease and Babesiosis:
Retrospective Review of First 3 Years’ Experience in One Medical Practice, Dr. Kenneth Liegner 2020
https://pubmed.ncbi.nlm.nih.gov/33291557/
Studies in Bb persister cells that led to studying disulfiram and the newer in vitro drug studies:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4576077/
https://www.ncbi.nlm.nih.gov/pubmed/26014929
Initial discovery of Disulfiram eradicating Persistent Lyme by Dr. Rajadas and Dr. VR Pothineni:
https://med.stanford.edu/news/all-news/2016/04/new-compounds-have-potential-to-combat-lyme-disease.html
Successful mouse study on Disulfiram for Persistent Lyme by Dr. Rajadas and his BioADD lab at Stanford:
https://www.biorxiv.org/content/10.1101/842286v1?rss=1
Columbia 2019-2021 clinical study on disulfiram:
https://clinicaltrials.gov/ct2/show/NCT03891667
Bay Area Lyme: The Disulfiram Story - by Bonnie Crater:
https://www.bayarealyme.org/blog/in-search-of-a-cure-for-lyme-disease-the-disulfiram-story/
Disulfiram (Tetraethylthiuram Disulfide) in the Treatment of Lyme Disease and Babesiosis: Report of Experience in Three Cases by Dr. Kenneth B. Liegner:
https://www.mdpi.com/2079-6382/8/2/72/htm?fbclid=IwAR2HFnDvVjTIjar4ig_KcDqmxW9OABbWOEeEfp_9MvaS2lWzjeMhHoJXf6I
“It is apparent from these data that B. burgdorferi bacteria, which have had time to adapt to their host, have the ability to escape immune recognition, tolerate the antibiotic doxycycline and invade vital organs such as the brain and heart,” said lead author Monica Embers, PhD, assistant professor of microbiology and immunology at Tulane University School of Medicine.
https://www.lymedisease.org/lyme-study-embers/
An excellent review of the literature on Bb persisters, that led to disulfiram being studied to kill persisters:
https://www.ncbi.nlm.nih.gov/pubmed/31097026
Peer-Reviewed Evidence of Persistence of Lyme Disease Spirochete Borrelia burgdorferi and Tick-Borne Diseases
The following is a list of over 700 peer-reviewed articles that support the evidence of persistence of Lyme and other tick-borne diseases. It is organized into different categories—general, neuropsychiatric, dementia and congenital transmission.
www.ilads.org/wp-content/uploads/2018/07/CLDList-ILADS.pdf
A note from Dr. Liegner on potential risks:
"I think this work is very important to be mindful of. Those of us who prescribe disulfiram and the patients who receive it must be aware of these significant toxicities/risks. It is a bit like cancer chemotherapy: it can help but also can harm. So dosages & durations need to be kept in mind, with vigilance for early detection of toxicities and cessation of the drug. Dr. Valentine's 'body of work' on disulfiram is very prodigious and insightful."
Here's the associated files to help educate you on the need for caution in using DSF as a treatment for Lyme and coinfections:
| dedc_toxicity_viquez_om_group_no_1_nihms50568.pdf |
| disulf_non-cs2_dependent_schwannopathy_rat_j_neuropath_exp_neurol_sept_2000.pdf |
| dedc_toxicity_viquez_om_group_no_3_nihms210174.pdf |
| dedc_toxicity_viquez_om_group_no_1a_nihms86653.pdf |
| dedc_toxicity_no_2_viquez_om_group_nihms-119853.pdf |
This website is maintained by the Texas Lyme Alliance. Visit our sister site for treatment information www.TXLymeAlliance.org. All donations made on either website are fully tax deductible per the IRS (FEIN# 85-0916055). Last updated 12/5/2020 with all of the newest information regarding disulfiram. Click the "contact" link to send us any inquiries or feedback. We are patient-centered and look forward to hearing from you. Join our newsletter for wellness information and calls to action to help better the lives of Lyme patients. We advocate for all ages around the globe to have a treatment that works! Thank you for visiting and God bless you all on your healing journey!
FB: @mkbauer6, @TexasLymeAlliance, @DisulfiramforLyme, @YogaSynergySpa
Twitter: @mkbauer6, @TexasLyme, @DisulfiramLyme,
Instagram: @mkbauer6
LinkedIn: www.linkedin.com/in/mkbauer6
https://youtube.com/c/KristinaBauer
FB: @mkbauer6, @TexasLymeAlliance, @DisulfiramforLyme, @YogaSynergySpa
Twitter: @mkbauer6, @TexasLyme, @DisulfiramLyme,
Instagram: @mkbauer6
LinkedIn: www.linkedin.com/in/mkbauer6
https://youtube.com/c/KristinaBauer
